")
")
 The figure (right) shows the screen of the LSFG system's analysis software. In this example, a blood flow map of the area called the optic nerve head of the human eye is being measured and displayed. The red areas represent the retinal blood vessel portions extending from the optic disc to the surrounding area. This blood flow map has a size of 750 x 360 pixels, runs at 30 frames per second, and can be observed continuously in real time — this is the greatest feature of this system that other devices cannot replicate. Click here to see the real-time changes of the blood flow map. The measurement area has been expanding year after year with improvements in the device, and currently the entire optic nerve head region can be observed in a single measurement. Software is also being improved to automatically stitch images together to observe an even wider area. The figure (below) shows the analysis of blood flow fluctuations within a single blood vessel; such measurements can also be easily performed.
The figure (right) shows the screen of the LSFG system's analysis software. In this example, a blood flow map of the area called the optic nerve head of the human eye is being measured and displayed. The red areas represent the retinal blood vessel portions extending from the optic disc to the surrounding area. This blood flow map has a size of 750 x 360 pixels, runs at 30 frames per second, and can be observed continuously in real time — this is the greatest feature of this system that other devices cannot replicate. Click here to see the real-time changes of the blood flow map. The measurement area has been expanding year after year with improvements in the device, and currently the entire optic nerve head region can be observed in a single measurement. Software is also being improved to automatically stitch images together to observe an even wider area. The figure (below) shows the analysis of blood flow fluctuations within a single blood vessel; such measurements can also be easily performed.

The figure below shows the appearance of the LSFG system, which consists of a fundus camera, a 3D stage, and a personal computer running measurement software and analysis software. Options may include an external fixation light and a motorized optical table. The laser uses near-infrared light, so compared to ordinary observation light illumination, there is virtually no stimulus to the eye. Under the class classification based on IEC60825-1, it has been classified as Class 1 by a third-party calibration organization, confirming its safety. In recent instruments, the fundus alignment is also performed using near-infrared light, making measurement even easier. The measurement is completed in just a few seconds, and the results can be saved as image files.
The figure below shows how the map size has evolved throughout the history of ophthalmic LSFG development.
In the early days, only a very small portion of the optic nerve head could be measured at one time, but with improvements to the instrument, the current LSFG-NAVI can capture the area from the optic nerve head to the vicinity of the macula in a single measurement.

The appearance of the device has also changed. From the first generation to the fourth generation, the configuration consisted of attaching a laser output unit and sensor unit to a fundus camera.
In the fifth generation, which obtained medical device certification, the camera unit became a dedicated unit.

When a frame does not contain normal data, it is called an error frame. The type of error frame is displayed in the Error Information bar at the bottom of the main form.
In most cases, it should display "TrackingErr."
In the case of tracking errors, there are broadly two reasons.
The first is an error due to fixational microsaccade detection. Frames in which fixational microsaccades occur move faster than the camera's shutter speed. Therefore, if such frames are included in the analysis, incorrect values may be produced. This function was introduced from Ver. 3. However, this detection function is not extremely accurate. In rare cases where errors appear at the rising phase of the heartbeat, it is highly likely that the detection is erroneous. If you wish to adjust this detection function, please edit the contents of "Sys.ini." This file should be located in the "C:\Program Files\Softcare.,Ltd\LSFG Analyzer" directory. Open the file and increase the value of "KOSHIBIDO_SHIKIICHI." This will make the detection function less sensitive. The value can be increased up to a maximum of 1. Setting the value to 1 disables this function.
The second reason is an error caused by exceeding the tracking movement limit.
This applies to cases where, for example, the optic disc was at the center of the screen at the start of measurement, but fixation could not be maintained afterward and the disc position shifted significantly to the right. The current tracking distance limit is 100 pixels relative to the reference frame. This is because tracking beyond that distance would likely result in areas with insufficient sample counts when creating HeartBeat or Composite maps.
MA, MV, and MT are three fundamental parameters used by LSFG-NAVI to classify the MBR (Mean Blur Rate: a relative index of blood flow velocity) within the optic nerve head (ONH) based on which region the MBR values are averaged over. Because they allow separate evaluation of blood flow in the overall, vascular, and tissue areas, they are extremely useful for assessing systemic circulation in healthy individuals and evaluating diseases such as diabetes and glaucoma. There are multiple methods for separating vascular and tissue blood flow depending on the purpose (e.g., Cross-sectional analysis, Histogram analysis, etc.).
LayerView Screen Appearance
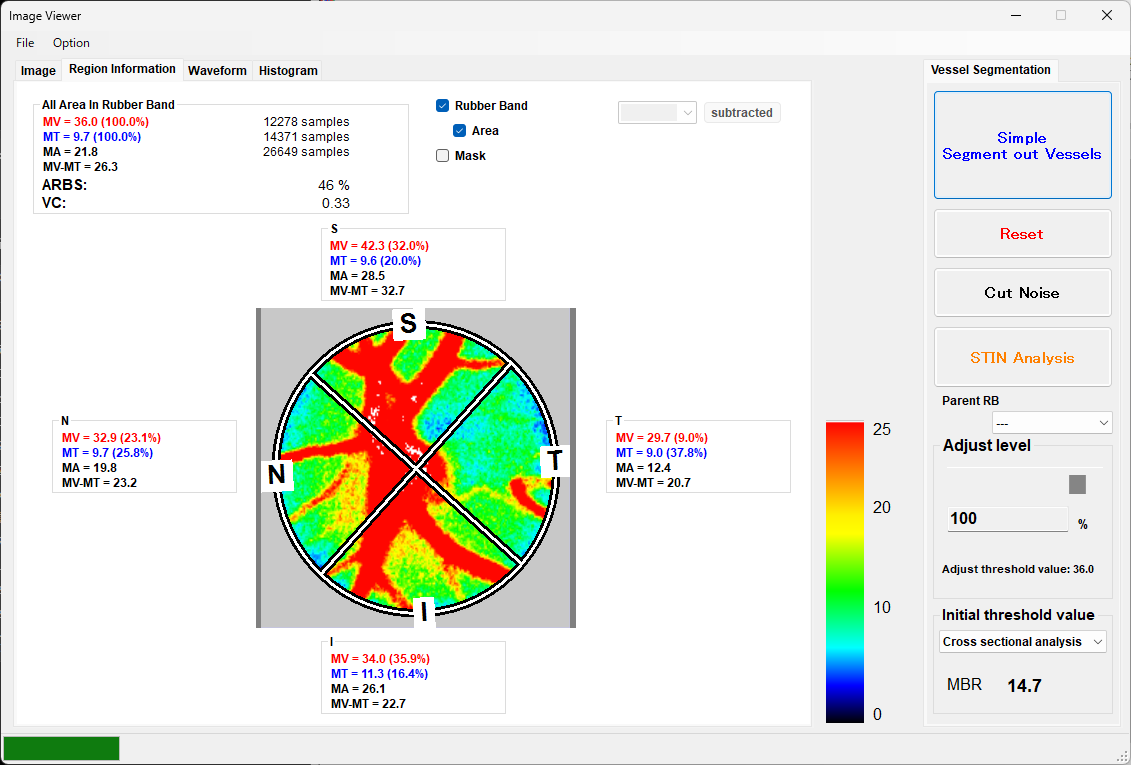
During STIN analysis, MV, MT, MA, and MV-MT are displayed for each of the superior/inferior/temporal/nasal sectors.
Meaning and Role of MA / MV / MT
In the ONH analysis of LSFG-NAVI, the area enclosed by the elliptical rubber band is automatically classified into vascular area and tissue area, and the MBR of each is averaged and quantified.
MA (Mean of All area)
-
The average MBR of the entire area within the rubber band (RB or ROI)
-
A comprehensive blood flow index combining vascular and tissue components
-
Used for an overall view of the blood flow status of the entire optic nerve head
-
Highly reproducible and one of the most commonly used indices in clinical research
In clinical use, the examiner can easily identify regions, and stable numerical values are obtained. In healthy individuals, the vascular area occupies approximately 40% of the entire optic disc. Since the vascular area has a higher MBR than the tissue area, it contributes significantly to MA. When the vascular area contracts, the proportion of the vascular area (referred to as ARBS) decreases, causing MA to decrease more than the actual change in blood flow. When blood flow through the large vessels decreases, MA responds more sensitively. For example, in cases where retinal large vessel blood flow is reduced due to arrhythmia, heart failure, etc., changes in MA become apparent.
MV (Mean of Vascular area)
-
The average MBR of the vascular area (retinal vessels)
-
Reflects blood flow in the vascular component within the optic nerve head
This includes the central retinal artery/vein and background tissue blood flow. Since the blood flow in the central retinal artery and vein is much greater than that in the tissue, the central retinal artery and vein blood flow is dominant.
-
Susceptible to the influence of vessel diameter and vascular density
-
Important for evaluating circulatory disorders
Since blood pumped from the heart flows directly through the ophthalmic artery and into the central artery, MV is considered to reflect blood flow dynamics on the central (proximal) side. The rubber band placed around the optic nerve head includes the central retinal artery and vein. The central retinal artery and vein are large vessels and have a large flow velocity distribution in the direction of the vessel diameter (cross-sectional and depth direction), so the MBR of the vascular area captured by the rubber band represents this varying velocity distribution. Originally, blood flow through a large vessel is expressed as cross-sectional area × average flow velocity, but since MV divides by the cross-sectional distance while maintaining depth information, MV is considered to be a value closer to average flow velocity rather than blood flow volume. In fact, there is a report1 showing a good correlation between MV and TRFI/W (TRFI, which is relative blood flow volume, divided by vessel width) (R2=0.615, p<0.0001). A high MV does not necessarily mean high blood flow volume in the retinal large vessels; a high MV may also indicate a narrow vessel diameter with high blood flow velocity. Since the central artery and vein are intermediate pathways for peripheral circulation, it may be better to focus on TRFI (the sum of RFV across retinal vessels extending beyond the disc) or changes in peripheral blood flow to capture actual blood flow volume.
MT (Mean of Tissue area)
-
The average MBR of the tissue area (optic disc tissue)
-
Reflects blood flow in the parenchyma of the optic nerve head (nerve fiber layer, glial tissue, etc.)
-
Allows evaluation of the circulatory status of tissue excluding vessels as blood flow volume (note: differences in pigmentation should be considered when comparing between individuals)
-
The relationship between glaucoma progression and structural changes in the ONH has been studied
MT represents blood flow supplied to the optic nerve head tissue area via the short posterior ciliary arteries branching from the ophthalmic artery. In contrast to MV, which represents blood flow on the central (proximal) side, MT represents blood flow on the peripheral (choroidal) side, enabling observation of the nutritional status provided by peripheral blood flow. Multiple reports2,3 show that MT correlates with absolute blood flow volume. The question of why MT correlates with blood flow volume arises from the difference between whether the detected pixels include the entire vascular structure or only a part of it. In the case of MT, each pixel contains multiple capillaries, meaning it observes multiple capillaries simultaneously. On the other hand, each pixel constituting MV represents only a part of the vascular structure, and each pixel constituting MV does not represent the blood flow of the target vessel as a whole. Since each pixel constituting MT already represents an average value that includes the capillary structure, the parameter MT, which averages these values, consequently correlates with the absolute blood flow volume of the target area.
What is MV-MT?
MV-MT is the value obtained by subtracting MT (tissue area blood flow) from MV (vascular area blood flow), and is a derived parameter for emphasizing the "vascular component dominance" within the optic nerve head.
Since the background tissue blood flow is subtracted, MV-MT is a parameter that captures changes in the central retinal artery and vein more sensitively than MV alone. As mentioned above, a high MV does not necessarily mean that MT also increases. Even when the effective blood flow volume is low (i.e., the blood flow volume reaching the peripheral side is low), there is a possibility that the artery contracts, increasing blood flow velocity and raising MV. In fact, while the pathways for MT and MV differ—the short posterior ciliary artery pathway and the central retinal artery pathway, respectively—comparing them in terms of peripheral versus central blood flow contrast should be meaningful.
In this context, MV-MT, which subtracts the tissue blood flow component MT, is considered a value that more closely reflects blood flow on the central (proximal) side.
Reasons for Using MV-MT
- To examine the balance between vascular and tissue components
The optic nerve head contains a mixture of vessels and tissue, and it is important to know how much blood flow each component accounts for. MV-MT shows this balance at a glance.
Potentially Useful for Disease Evaluation
Research has reported tendencies for MT to decrease in conditions such as:
-
Glaucoma
-
Optic neuropathy
-
Circulatory disorders
On the other hand, a study7 analyzing the factors contributing to individual differences in MV and MT in normal eyes has shown that MT and MV are independent circulatory indices. The fact that MT and MV are independent means that MV-MT can be used as an index for relatively capturing the decline in tissue blood flow.
■ Definition
In other words:
-
How much higher the vascular blood flow is compared to the tissue
-
An index that quantifies the dominance of vascular blood flow (the "distribution dominance" of large vessels and the "anatomical dominance/nutrient vessels")
Comparison of the Four Parameters
| Parameter | Target Area | Meaning | Primary Use |
|---|---|---|---|
| MA | All areas | Blood flow of the entire optic nerve head | Overall evaluation, high reproducibility |
| MV | Vascular area | Retinal vessel blood flow (central/proximal side, reflecting central retinal artery and vein) | Evaluation of vascular component circulation |
| MT | Tissue area | Optic disc tissue blood flow (peripheral side, supplied from the short posterior ciliary arteries on the choroidal side, reflecting tissue blood flow) | Tissue circulation, glaucoma evaluation |
| MV-MT | Vascular area |
Retinal vessel blood flow (excluding background tissue blood flow) |
CRVO4,5, BRVO, optic neuropathy, systemic circulation central-side evaluation, circulatory disorders |
Clinical Points
● High Reproducibility
MA, MV, and MT have all been reported6 to have high intra-examiner and inter-examiner reproducibility. (e.g., in the glaucoma group: MA CV=5.3%, MV CV=4.2%, MT CV=2.5%)
-
In glaucoma, the decrease in MT (tissue blood flow) is particularly notable
-
There are also reports suggesting that changes in the tissue area (MT) may correlate with structural changes more than the vascular area (MV)
● Combined Use with Pulse Waveform Analysis
MT and MV are also used in pulse waveform analysis (such as Blowout Score), enabling more detailed evaluation of the circulatory dynamics of the optic nerve head7
Methods for Separating Vascular and Tissue Blood Flow
- Cross-sectional analysis
- A method that preferentially extracts tissue blood flow (MT): Used when stable extraction of peripheral tissue blood flow is desired. Suitable for diseases such as glaucoma and for observing peripheral blood flow dynamics in healthy individuals.
- Histogram analysis
- A method that preferentially extracts the vascular area (MV): Used when stable extraction of large vessels with minimal tissue blood flow interference is desired. Histogram analysis is used when calculating TCR, which measures peripheral vascular resistance from large vessels. Suitable for diseases where TCR is utilized, such as CRVO, BRVO, age-related arteriosclerosis, and for observing blood flow dynamics of the larger vessels in healthy individuals.
- Manual
- Used when manually delineating vascular and tissue areas. This method divides the MBR within the rubber band placed on the optic nerve head using a single threshold value. Pixels with MBR above the threshold are classified as vascular, and those below as tissue blood flow for calculation.
References
- Michelle R. Tamplin, Kimberly A. Broadhurst, Anthony H. Vitale, Ryuya Hashimoto, Randy H. Kardon and Isabella M. Grumbach
Longitudinal Testing of Retinal Blood Flow in a Mouse Model of Hypertension by Laser Speckle Flowgraphy
Translational vision science & technology, 10(2), 16-16, doi:10.1167/tvst.10.2.16, 2021. [Link] - Hiroaki Takahashi, Tetsuya Sugiyama, Hideki Tokushige, Takatoshi Maeno, Toru Nakazawa, Tsunehiko Ikeda, Makoto Araie
Comparison of CCD-equipped laser speckle flowgraphy with hydrogen gas clearance method in the measurement of optic nerve head microcirculation in rabbits
Experimental Eye Research(2012), http://dx.doi.org/10.1016/j.exer.2012.12.003 doi:10.1016/j.exer.2012.12.003 [Link] - Naoko Aizawa, Fumihiko Nitta, Hiroshi Kunikata, Tetsuya Sugiyama, Tsunehiko Ikeda, Makoto Araie and Toru Nakazawa
Laser speckle and hydrogen gas clearance measurements of optic nerve circulation in albino and pigmented rabbits with or without optic disc atrophy.
Investigative Ophthalmology & Visual Science, IOVS-14, 2014. doi: 10.1167/iovs.14-15373 [Link] - Matsumoto Makiko, Suzuma Kiyoshi, Fukazawa Yoshiko, Yamada Yoshihisa, Tsuiki Eiko, Fujikawa Azusa and Kitaoka Takashi
Retinal blood flow levels measured by Laser Speckle Flowgraphy in patients who received intravitreal bevacizumab injection for macular edema secondary to central retinal vein occlusion.
Retinal Cases and Brief Reports, 8(1), 60-66, 2014. doi:10.1097/icb.0000000000000005 [Link] - Makiko Matsumoto, Kiyoshi Suzuma, Fumito Akiyama, Kanako Yamada, Shiori Harada, Eiko Tsuiki and Takashi Kitaoka
Retinal Microvascular Resistance Estimated from Waveform Analysis Is Significantly Higher With a Threshold Value in Central Retinal Vein Occlusion
Translational Vision Science and Technology, 9(11), 4, doi:10.1167/tvst.9.11.4, 2020. [Link] - 小川 莉奈、斎藤 彩、江黒 友春、永野 幸一、山口 純、庄司 信行
レーザースペックルフローグラフィーにおける視神経乳頭血流の再現性および一致性
日本視能訓練士協会誌, 50, 129-134, doi:10.4263/jorthoptic.50F115, 2022. - Ayako Anraku, Nobuko Enomoto, Goji Tomita, Aiko Iwase, Takashi Sato, Nobuyuki Shoji, Tomoaki Shiba, Toru Nakazawa, Kazuhisa Sugiyama, Koji Nitta and Makoto Araie
Ocular and Systemic Factors Affecting Laser Speckle Flowgraphy Measurements in the Optic Nerve Head
Translational Vision Science & Technology, 10(1), 13, doi:10.1167/tvst.10.1.13, 2021. [Link]
Revision:20260211
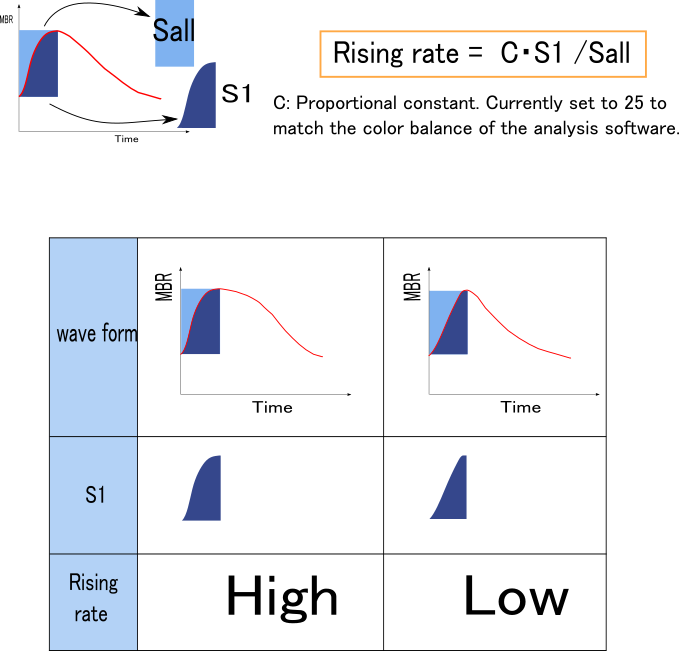
While other indices such as Skew and BOS quantify the shape of the entire waveform,
Rising Rate and Falling Rate focus on the ascending and descending portions of the heartbeat waveform, respectively.
In a word, Rising Rate is a quantification of how mild the blood flow rise is. A healthy heart produces a mild blood flow rising waveform, but in conditions such as heart failure, the waveform appears to rise steeply. Therefore, Rising Rate increases when the waveform is mild. It appears to be a value that is not dependent on age.
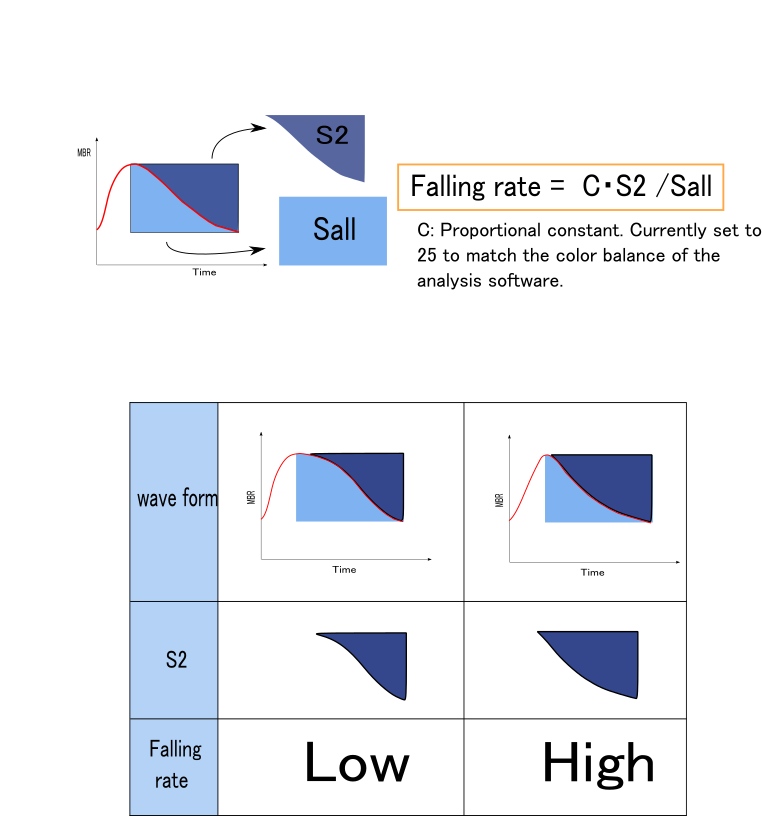
On the other hand, Falling Rate focuses on the waveform after the peak and, in a word, represents how quickly the blood flow recedes. As age increases, the peripheral vessels decrease, and the blood flow that filled the peripheral side quickly subsides like a receding tide. In this case, Falling Rate becomes higher. Conversely, when there is an abundant peripheral vascular bed, the flow recedes slowly and blood flow transitions gradually to the diastolic phase. For this reason, Falling Rate correlates well with age and shows a positive correlation.
As shown in the figure below, the ratio of the areas before and after the peak of the waveform is represented.
Like Skew, this index becomes larger when the rise/fall is rapid and smaller when it is gradual.
Rising Rate
Falling Rate
Recent Reports
- Tomoaki Shiba, Mao Takahashi, Tadashi Matsumoto and Yuichi Hori
Pulse Waveform Analysis in Ocular Microcirculation by Laser Speckle Flowgraphy in Patients with Left Ventricular Systolic and Diastolic Dysfunction
Journal of vascular research, 55(6), 329-337, doi:10.1159/000494066, 2018.